| Disease | Alb | PZQ | IVM | AZM | DEC | MOX | Other |
|---|---|---|---|---|---|---|---|
| STH | ✓ | MBD | |||||
| Schisto | ✓† | ✓ | OXA | ||||
| LF | ✓† | ✓ | ✓ | ✓ | DOX* | ||
| Trachoma | ✓‡ | ✓ | TEO |
Accounting for the impact of mass-drug administration for NTDs prevalence mapping using geostatistical methods
A decay-adjusted spatio-temporal (DAST) model
Neglected tropical diseases
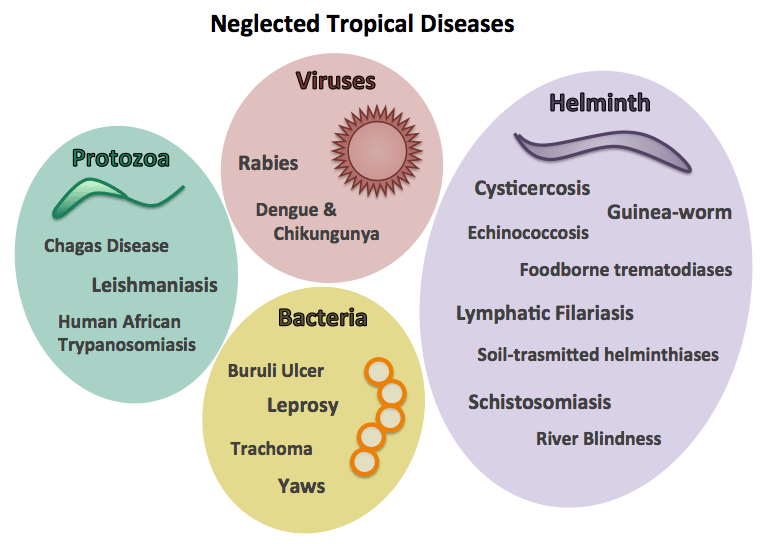
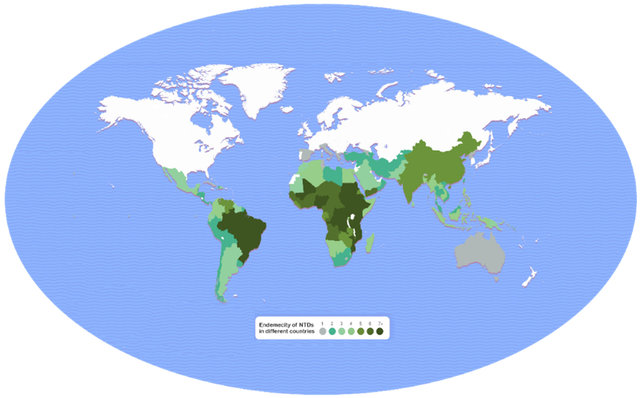
NTD endemic areas
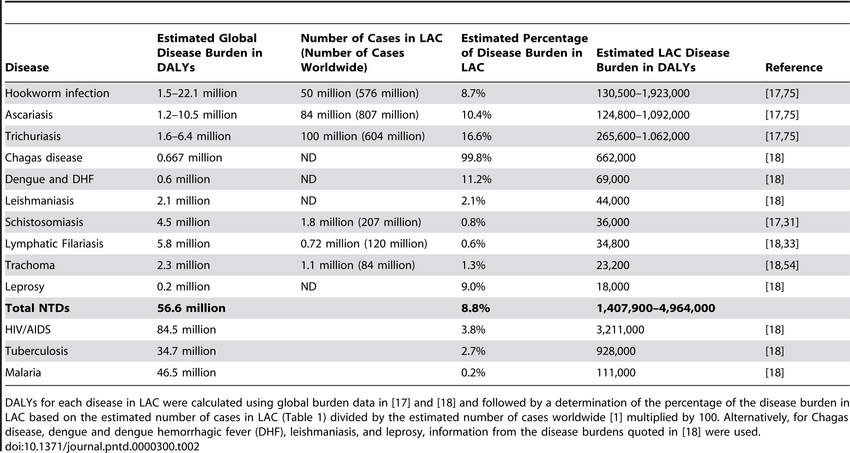
The impact of NTDs
NTDs Risk Factors


Common risk factors:
- Poor sanitation and lack of clean water
- Limited healthcare access
- Poverty and overcrowding
- Exposure to disease vectors (e.g., mosquitoes, flies)
- Lack of education and awareness
Albendazole
How it works:
Albendazole disrupts the metabolism of parasitic worms by inhibiting microtubule formation, which is essential for their survival.
Used for NTDs such as:
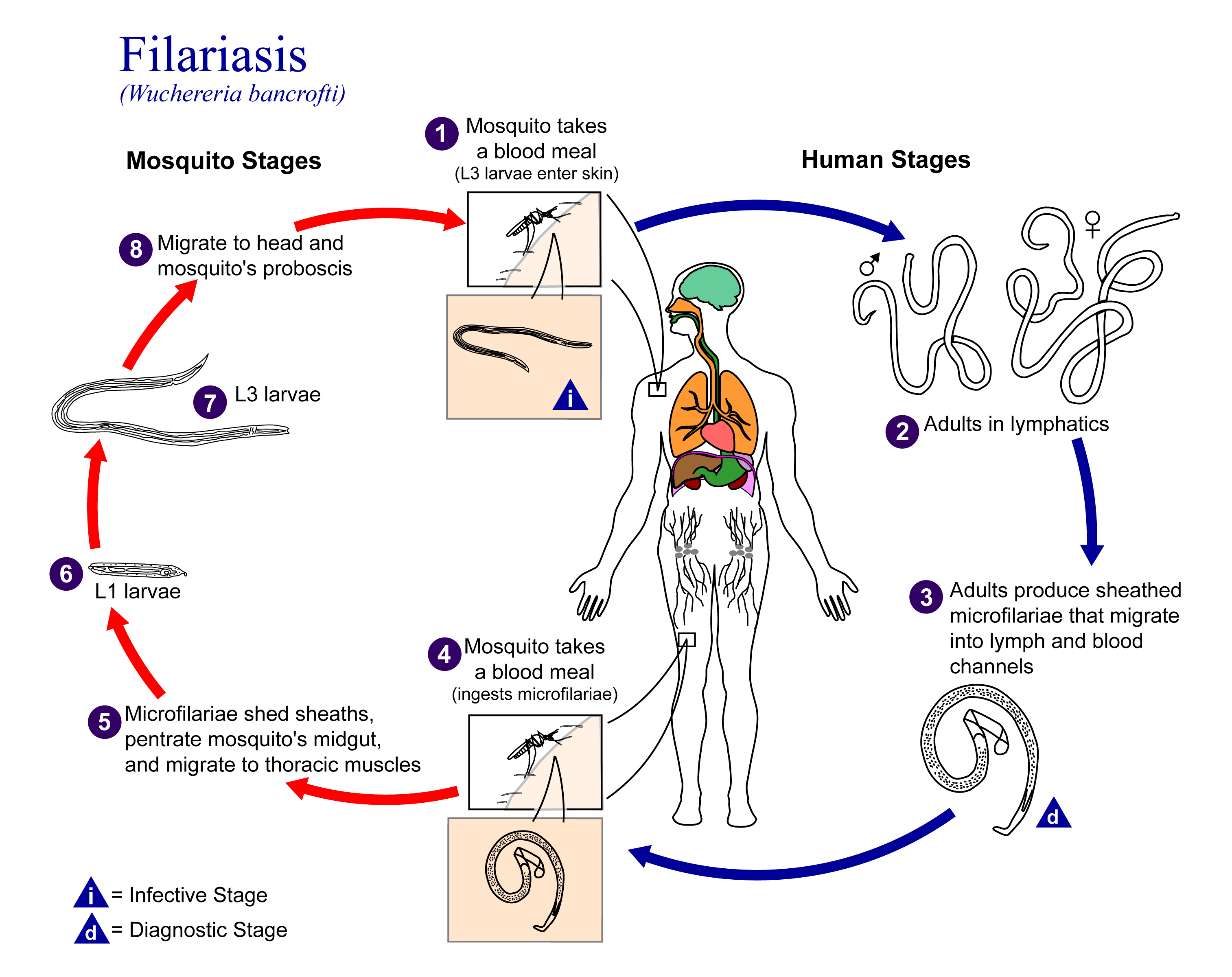
Lymphatic filariasis (in combination with ivermectin or DEC)
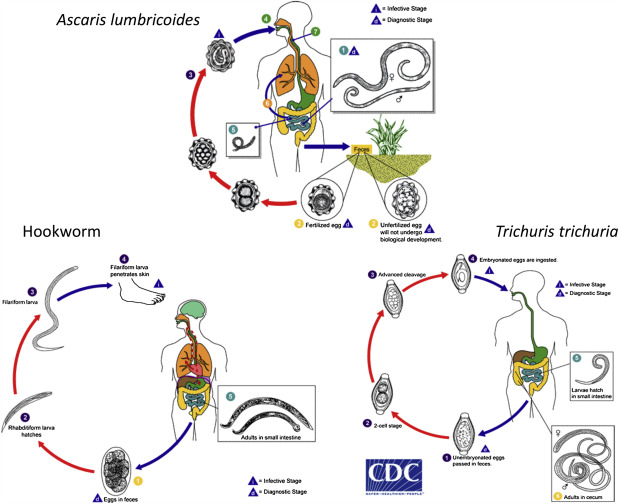
Soil-transmitted helminths (e.g., ascariasis, hookworm, trichuriasis)
MDA use:
Distributed in large-scale deworming campaigns, particularly targeting children and at-risk communities.
Ivermectin

How it works:
Ivermectin paralyzes and kills parasites by interfering with their nerve and muscle function via chloride channel disruption. Parasites cannot move and feed.
Used for NTDs such as:
Onchocerciasis (river blindness)
Lymphatic filariasis (in combination with albendazole)
Strongyloidiasis
MDA use: Ivermectin is given to both adults and children (weighing more than 15kg), but its use is carefully considered for pregnant women.
Praziquantel

How it works:
Praziquantel increases permeability of the parasite’s cell membranes to calcium ions, causing muscle contraction and paralysis.
Used for NTDs such as:
Schistosomiasis
Tapeworm infections
MDA use:
Key drug in school-based and community-wide treatment campaigns in regions with high schistosomiasis burden.
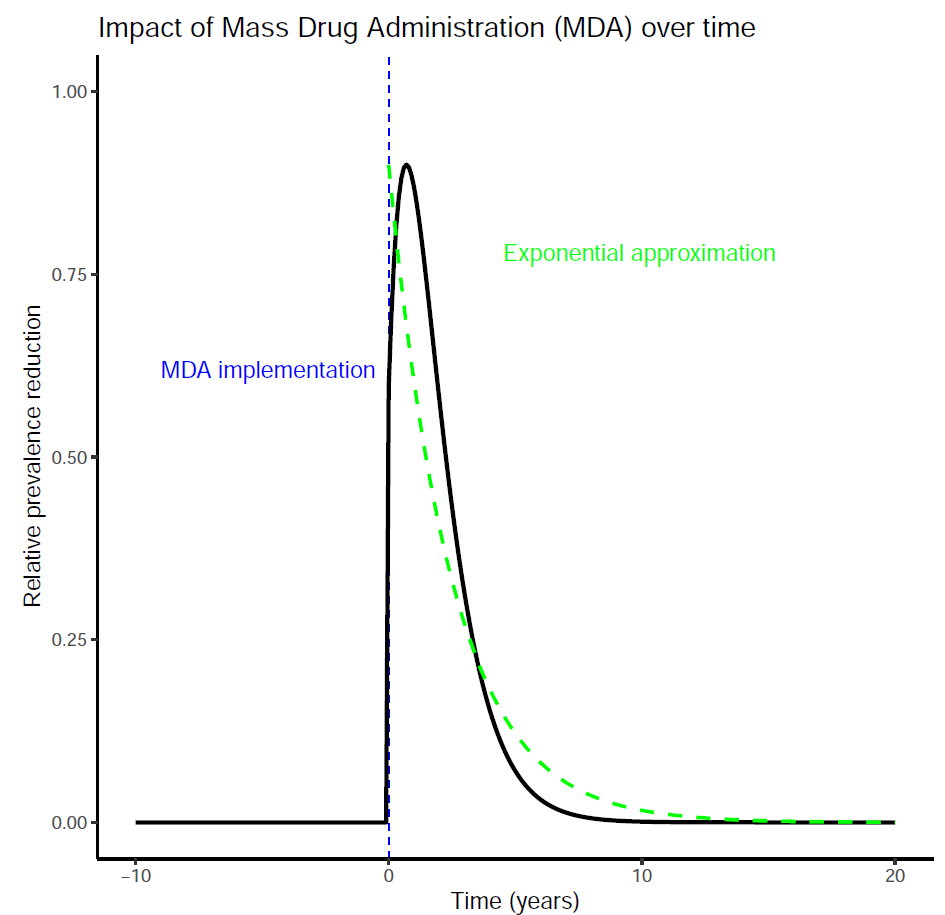
Modelling the impact of MDA
Spatial and temporal confounding with MDA
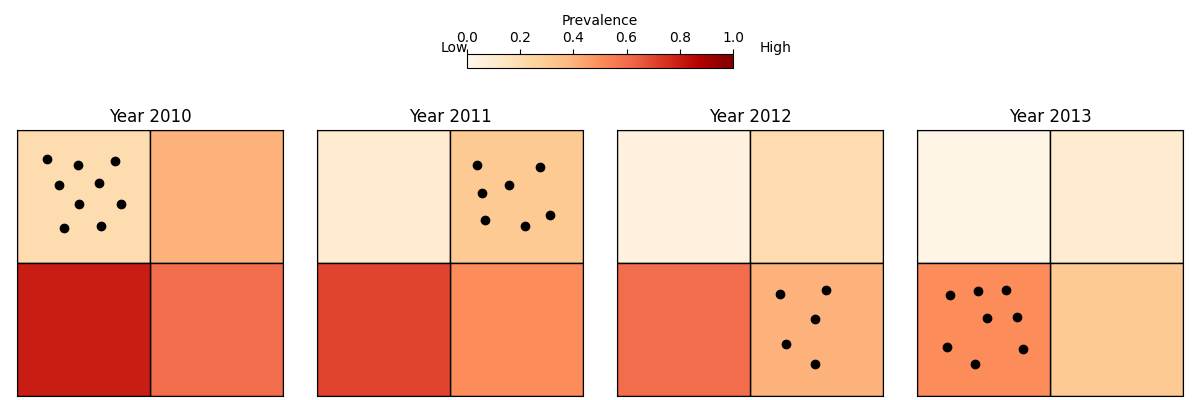
Issues:
Areas with different levels of transmission are sampled at different times.
Use of MDA rounds can even show a positive associated with disease risk
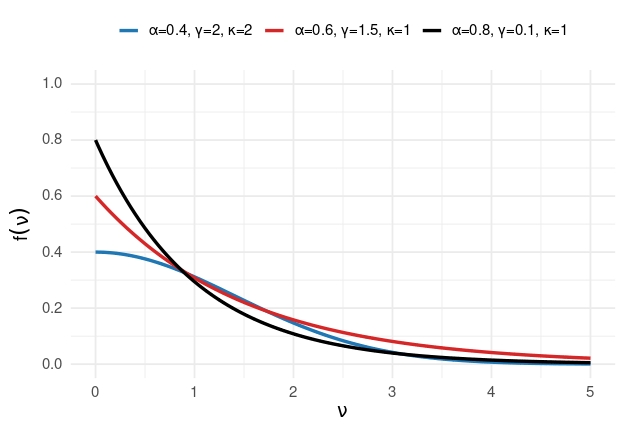
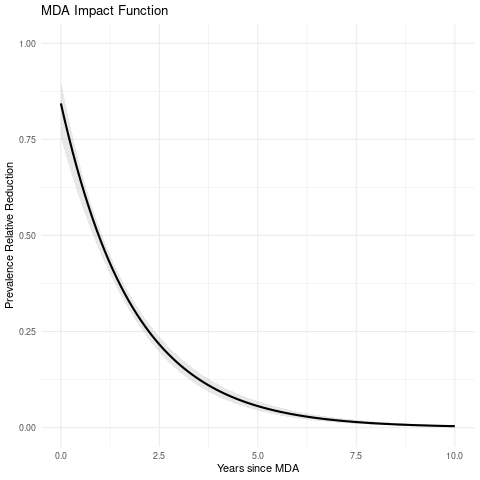
Parametric form of MDA decay function
\[f(v) = \alpha \exp\left\{ -\left(\frac{v}{\gamma}\right)^{\kappa} \right\}\]
- \(\alpha\): maximum reduction immediately after MDA
- \(\gamma\): scale of decay
- \(\kappa\): shape of decay (fixed)
Monte Carlo Maximum Likelihood
- Let \(W_i = S(x_i) + Z_i\) and \(W = (W_1, \ldots, W_n)\)
The likelihood function for parameters \(\theta = (\beta, \sigma^2, \phi, \tau^2)\) is given by:
\[L(\theta) = \int N(W; D\beta, \Omega) f(y| W) dW\]
where \(\Omega = \sigma^2 R(\phi) + \tau^2I_n\).
We approximate this using Monte Carlo integration:
\[L_m(\theta) = \frac{1}{B} \sum_{j=1}^{B} \frac{N\left(W^{(j)}; D\beta, \Omega \right)}{N\left(W^{(j)}; D\beta_0, \Omega_0\right)}\] where \(W^{(i)}\) are sampled from the distribution of \(W\) given \(y\) using an MCMC algorithm.
All implemented in the
dastfunction of theRiskMappackage
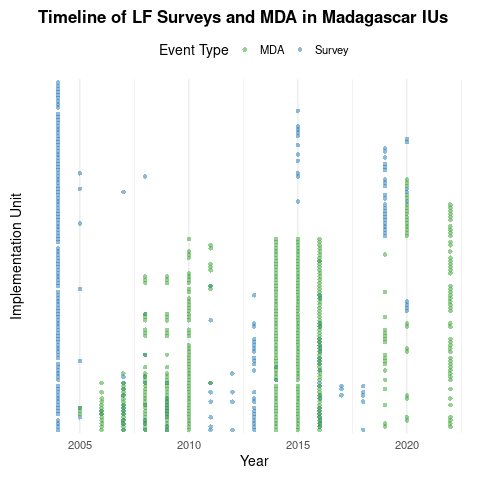
Example: Lymphatic filariasis in Madagascar
Timeline of surveys and MDA
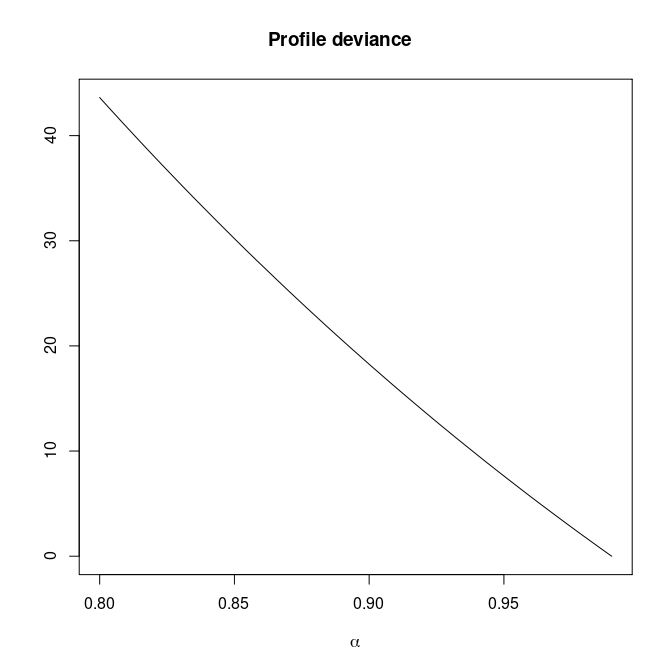
Monotone likelihood for \(\alpha\)
Introducing penalization for \(\alpha\)
- Let \(p(\alpha) > 0\) be a positive function.
- The penalized likelihood for \(\alpha\) is \[L_{p}(\theta) = L(\theta) - p(\alpha)\]
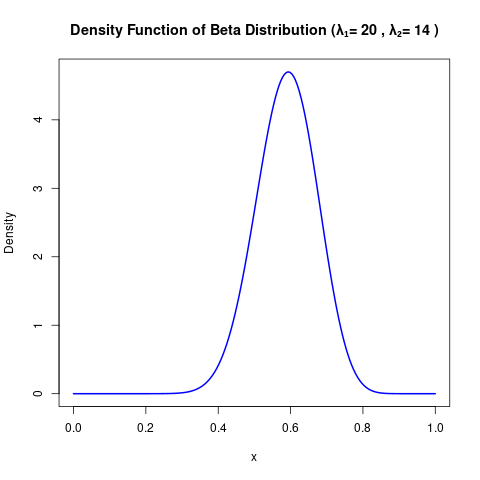
Proposed penalty
\[p(\alpha) = -\left[\lambda_1 \log\alpha + \lambda_2\log(1-\alpha) \right]\]
- We set \(\lambda_1 = 20\) and \(\lambda_2 = 14\). (This inspired by a Beta distribution with mode in around 0.6, with 0.42 and 0.7 as its 0.025 and 0.975 quantiles, respectively.)
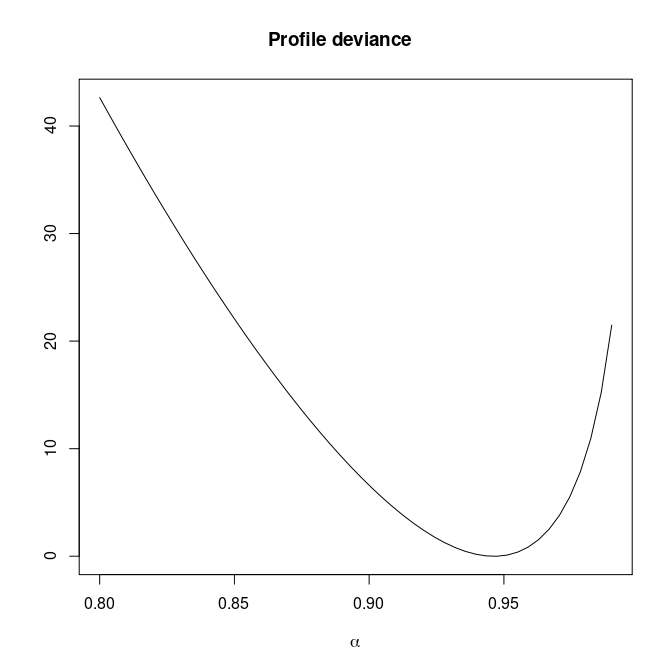
Introducing penalization for \(\alpha\)
Estimated MDA impact function
Prevalence prediction 2000-2024
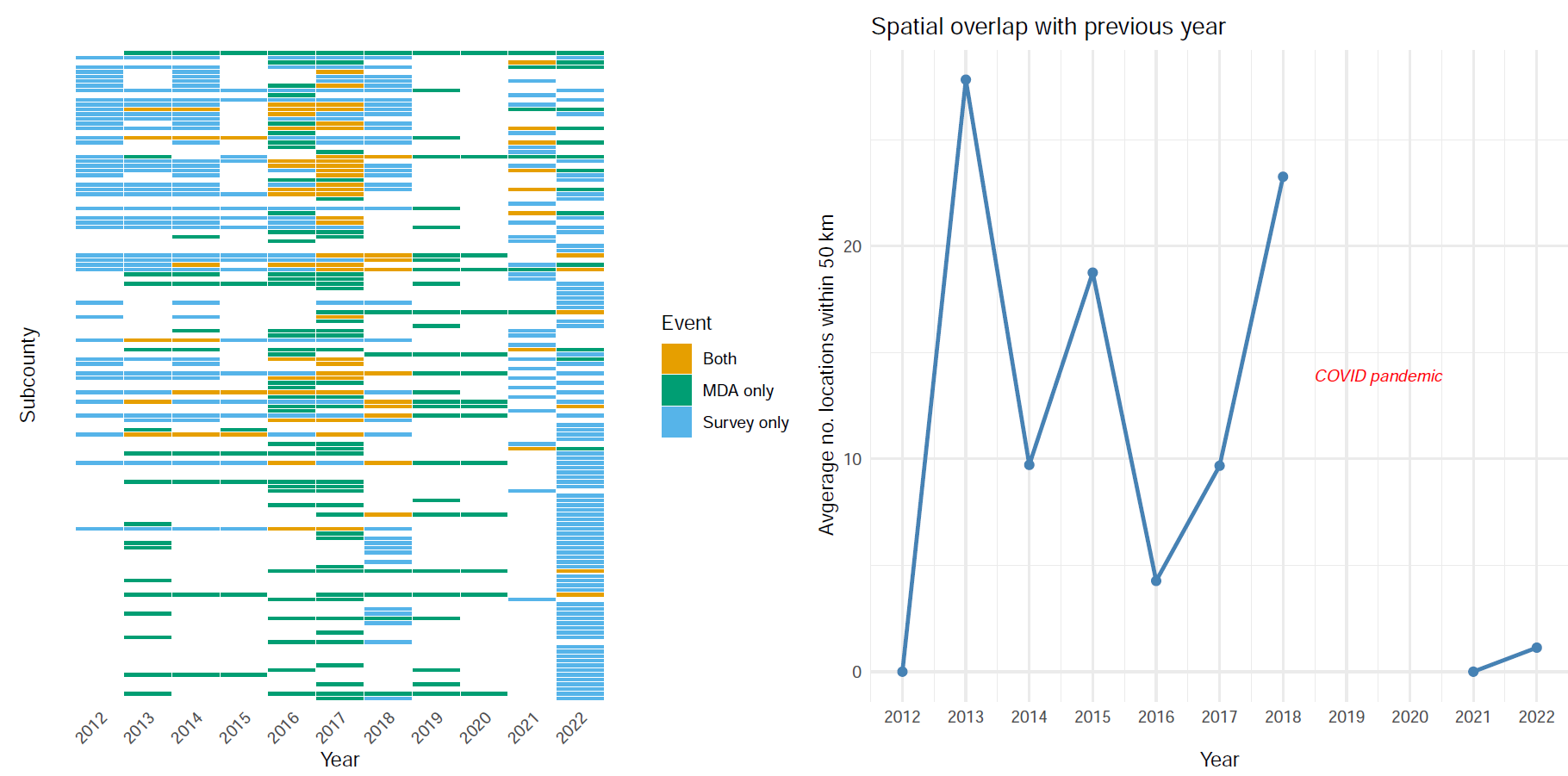
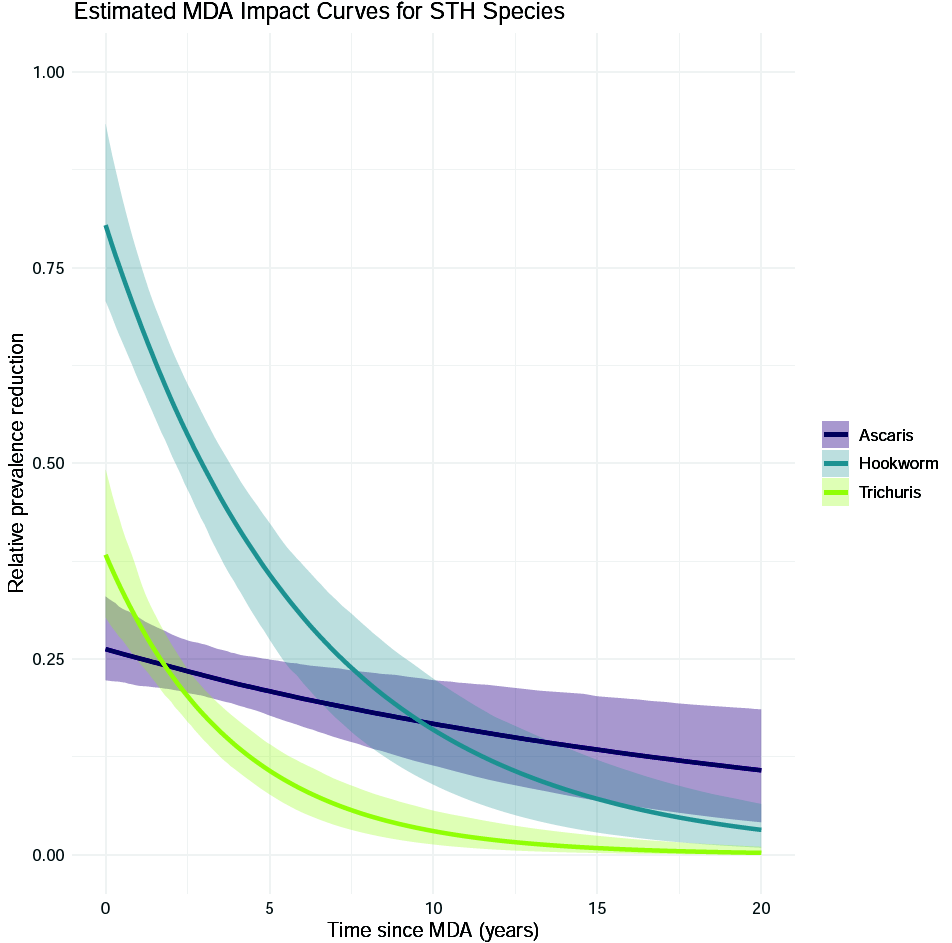
Example: soil-transmitted helminths in Kenya
Timeline of surveys and MDA
The MDA impact by STH species
Prevalence prediction 2012-2023
THANK YOU!

🔗 giorgistat.github.io
📧 e.giorgi@bham.ac.uk
📍 Department of Applied Health Sciences, University of Birmingham